![]()
|
|
Top Previous Next |
|
Bayesian analysis
Introduction The selection of a drug dosage regimen in the absence of measured drug levels (ie., a priori drug dosing) is based on estimates of the patient's pharmacokinetic parameters adjusted for patient characteristics (ie., weight, age, sex, serum creatinine). This is also referred to as population kinetics. An example of a priori kinetics is the Hull and Sarrubi nomogram for aminoglycoside dosing.
The traditional use of measured drug levels (ie., a Posteriori drug dosing) is to estimate the patient's pharmacokinetic parameters from the measured drug levels without relying in any way on the population kinetics. An example of a Posteriori dosing is the Sawchuk and Zaske method for aminoglycoside dosing.
The Bayesian approach incorporates both sets of data for estimating the patient's pharmacokinetic parameters. It uses the a priori pharmacokinetic parameters of the population as the starting estimate for an individual; it then adjusts these estimates based on the patient's measured drug levels taking into consideration the variability of the population parameters and the serum level data. A priori information is not discarded, but it is appropriately incorporated into the estimation procedure. The appeal of this approach is that is mimics human thinking. That is, the result of any clinical test should be interpreted in light of both the a priori expectations and knowledge of the variability of the test itself.
Precautions
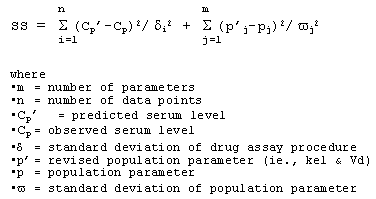
Pharmacokinetic formulas The Bayesian approach estimates pharmacokinetic parameters (e.g., kel /CL and Vd) that will be most consistent with serum levels predicted by both the population model and the actual measured serum levels. To achieve that end, the least squares method based on the Bayesian algorithm estimates the parameters which minimize the following function:
The program will display the initial and final sum of residual squares (SS) and the number of iterations required to minimize the SS.
Standard deviation of population parameters After correcting for age, weight, sex, and renal function there is a coefficient of variation of population pharmacokinetic parameters that is on the order of 20-50%. In the aminoglycoside model, 40% is used as the default value for the variability for both clearance and distribution volume. In the vancomycin model, the default variability for clearance is 40%, the default distribution volume variability is 20%.
Standard deviation of drug assay procedure A reasonable coefficient of variation of serum assay error is on the order of 5 to 15%. According to published data, serum assay error patterns are well represented by a second order polynomial: SAE = SD1+ (SD2 * Cp) + (SD3 * Cp^2)
Weighting of serum level data Individual data points are then weighted according to the serum assay error (SAE), a fixed variability (SD4) which accounts for environmental errors, and the time from dose administration (Time) which gives more weight to the trough level: Weight(i) = 1 / [ {Cp(i) * SAE + SD4} * {1.005 ^ [Interval - Time(i)] } ] ^ 2
|
. ©Copyright 1999 - 2025, by RxKinetics. All rights reserved.