This update was long overdue. It has been nearly two years since the last significant update and a lot has changed since then. I’ve been on a sabbatical of sorts from programming since last summer when I retired from the full-time hospital pharmacy grind. I’ve spent the time since decompressing and mulling over what I could do to make the program more intuitive and relevant to current practices.
The highlights of version 2.3.26 are:
- Added Targeted AUC dosing.
- Replaced the DripCharts button with a Targeted AUC button.
- Improved the settings dialog adding height/weight and SrCr options.
- Disabling update checks on the settings dialog also disables all internet access (More models).
- Increased max weight to 299 kg (obesity epidemic).
- Levels outside the dosing interval are now allowed to accommodate late draws.
- Added free text infusion time to Retrospective dosing.
- Clarified checks to the 2- and 3- point analysis.
- Updated Bayesian for 2- and 3- point analysis.
- Improved AUC calculations (log-trap and bedside).
- Improved Other CrCl calculations for IDMS CREAT and fixed Jelliffe multi-step.
- Replaced the save to PDF function with ‘Copy consult to clipboard’ for pasting into the eMR.
- Fixed some quirks on the consult print-out.
- Update the Blank_PK_monitor.doc to include precautions.
- Updated the accompanying help file.
Targeted AUC dosing
I tried to make the biggest change as obvious as possible by replacing the (seldom used) DripCharts toolbar button with a Targeted AUC button:

After selecting and calculating a Vancomyicn model (either prospective or retrospective), the Targeted AUC button becomes active and when clicked, takes you to the AUC dosing dialog:
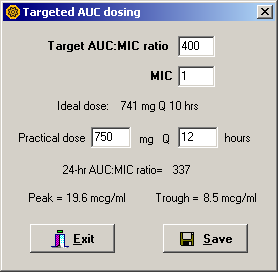
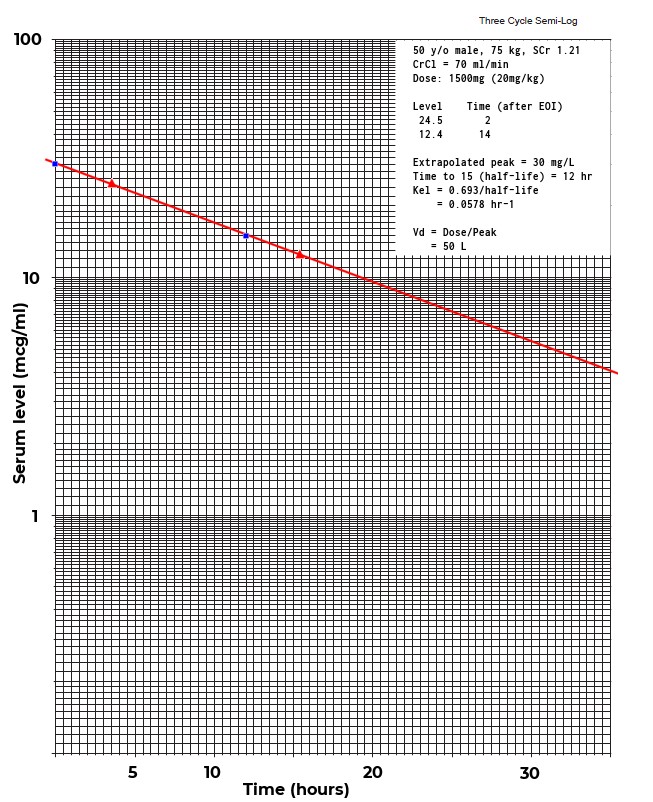
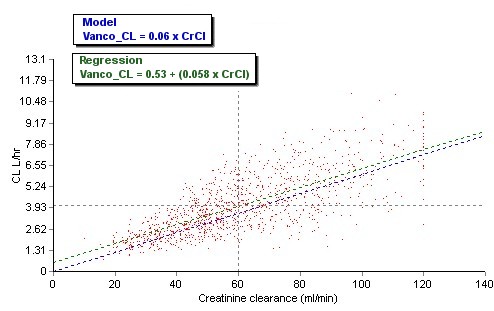
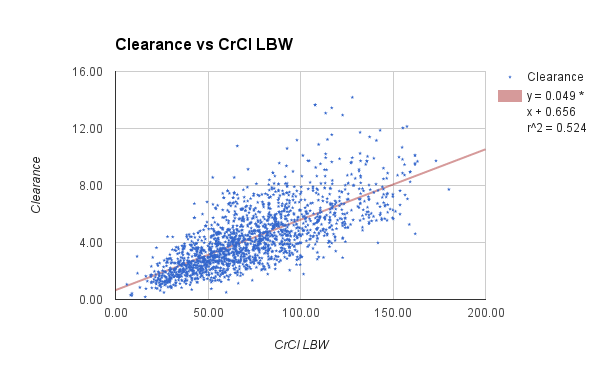
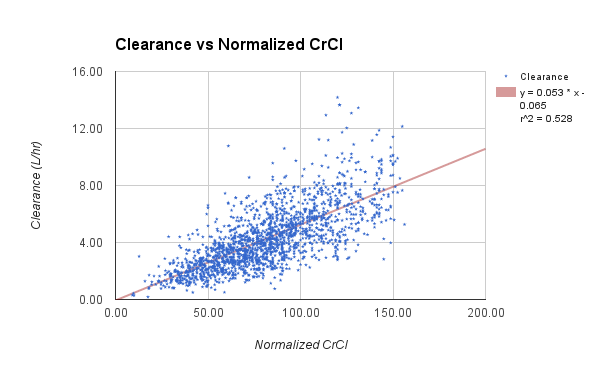
Targeted AUC dosing takes advantage of the fundamental relationship between clearance, dose and AUC that we all learned in basic pharmacokinetics class:
AUC = Dose (mg/hr) ÷ CL (L/hr)Simply rearrange this equation to solve for dose:
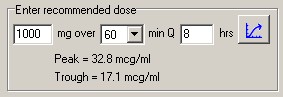
Dose (mg/hr) = AUC x CLSince dosing at the half-life is ideal for Vancomycin, the initial interval selected by AbPK is the estimated half-life plus the infusion time (rounded to the nearest whole number). The dose then is:
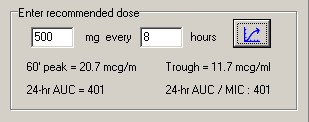
Dose (mg) = Dose (mg/hr) x Interval (hr).The ideal interval and dose thus calculated are usually not practical, and are only meant to be a starting point. You must use your clinical judgment to select an appropriate dose to reach the target AUC.
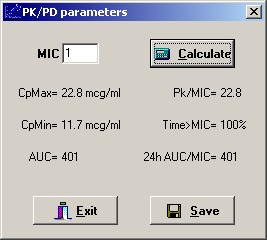
Once a dose and interval are chosen, the AUC/MIC is calculated along with the expected peak and trough. Click the Save button to copy this information to the main program.
Copy consult to clipboard
In my opinion this is the second most important change in the latest version. We all work with the eMR now and it seems silly to still be printing hard copies of consults. This function will create a text summary of your pk consult and copy it to the Windows clipboard. You can then paste it into your eMR consult note by using the standard Windows paste shortcut: Ctrl+V.

Internet access
IS types are understandably paranoid about any application that accesses the internet. Disabling update checks on the settings dialog will disable all internet access by AbPK.

Sample time limits
Previous versions of AbPK had hard-coded stops on draw times, which I admit were short-sighted. Busy lab/nursing personnel don’t always draw serum levels at the optimal time. AbPK will now accept draw times that are outside the dosing interval.
Hints
Nothing new, but wanted to throw this out there. Please remember that hover hints are everywhere. Pause your mouse pointer for a second to see more details from the underlying information display. For example hover your mouse over the dose entry to view mg/kg. Pause your mouse over the Pk results frame to view time to steady-state. Hover your mouse over the serum level entry boxes to view more details. etc. etc.
Free as in beer
As always updates are free, downloaded from the web site using the web update function.